Liang Xu,
Bing Zhao,
Jing Sun,
Hai-ping Wang,
Rong Wang ![]()
For correspondence:- Rong Wang Email: wangrong133494@163.com Tel:+8653168777061
Received: 9 May 2015 Accepted: 11 February 2016 Published: 31 March 2016
Citation: Xu L, Zhao B, Sun J, Wang H, Wang R. Clematis chinensis extract protects against diabetic nephropathy in rats. Trop J Pharm Res 2016; 15(3):513-519 doi: 10.4314/tjpr.v15i3.12
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To study the effect of Clematis chinensis extract (CCE) on diabetic nephropathy in rats.
Methods: Eight-week old male Wistar rats were injected with streptozotocin to induce diabetes. The effects of CCE(250 or 500 mg/kg) on renal function index, fasting blood glucose (FBG), blood fat, oxidation index, and pathological kidney changes for 3 weeks were compared to those of the positive control drug, captopril.
Results: At 12 weeks, CCE(500 mg/kg) treatment had significantly decreased serum blood urea nitrogen (BUN, 12.61 ± 1.42 mmol/L), serum creatinine (SCr, 84.64 ± 6.37 μmol/L), creatinine clearance (CCr, 0.88 ± 0.10 mmol/L), interleukin-6 (IL-6, 297.56 ± 19.62 pg/mL), urinary albumin, urinary albumin excretion rate (UAER, 11.68 ± 0.97 μg/min), kidney hypertrophy index (kidney weight/body weight, 0.58 ± 0.03%) and FBG (11.51 ± 0.96 mmol·L-1). It significantly decreased triglyceride (TG, 0.26 ± 0.05 mmol/L), total cholesterol (TC, 1.52 ± 0.06 mmol/L) and low-density lipoprotein-cholesterol (LDL-c, 0.71 ± 0.06 mmol/L) levels and increased high-density lipoprotein-cholesterol (HDL-c, 0.65 ± 0.05 mmol/L). CCE treatment also significantly decreased malondialdehyde (MDA, 16.14 ± 1.24 nmol/mgprot) levels and increased superoxide dismutase (SOD, 95.17 ± 4.06 U/mgprot) and glutathione peroxidase (GSH-Px, 154.33 ± 11.76 mmol/L) (both p < 0.05). Finally, CCE reduced the degree of glomerular basement membrane and renal tubular thickening and swelling in diabetic rats.
Conclusion: CCE has a significant inhibitory effect on diabetic nephropathy-induced renal injury in rats.
Introduction
Diabetic nephropathy (DN) is a frequent and major microvascular complication of diabetes mellitus and is the most common cause of end-stage renal failure disease in many countries [1]. Several factors such as hyperglycemia, hyperlipidemia, oxidative stress, and inflammatory cytokines contribute to renal damage progression in DN. While both types 1 and 2 diabetes mellitus can lead to DN, it is more common with the latter [2]. DN is characterized by glomerular and tubular hypertrophy, basement membrane thickening, extracellular matrix component accumulation, glomerulosclerosis, and tubulo-interstitial fibrosis in the mesangium and interstitium [3].
Traditional herbal medicines are widely used in different countries. Medicinal plants are used as therapies for multiple diseases including DN [4,5]. For example, Sefi et al showed that Artemisia campestris leaf extract prevented DN by attenuating oxidative and nitrosative stress [6]. It was reported that Clematis chinensis could improve kidney damage and exert significant protection against DN [7,8]. The aim of this study was to examine the effect of CCE on DN progression in high-fat diet and streptozotocin (STZ)-induced diabetic rats.
Methods
Material
Herbal samples of Clematis chinensis were collected from Bozhou City, Anhui Province in China in July 2014. The taxonomic identification of the plant was performed by Professor Jin-ke Liu of the pharmacy department at Shandong University, China. A voucher specimen (No. CCE 201308024) was deposited in the herbarium of Shandong University, China for future reference.
Three batches of Clematis chinensis were dried in an oven, and an aqueous extract was obtained by steeping the dried herb in water at 60 °C for 3 h. The extracted fluid was dried in an oven and freeze-dried; 1 g powder was equivalent to about 1.8 g of the plant (53.28 % yield).
Animals and grouping
Eight-week-old male Wistar rats (weighing 300–350 g) were provided by the Experimental Animal Center of Shandong Province (Certificate no. SYXK2004-0003). The animals had free access to feed and water and were allowed to acclimatize for at least 1 week before use. The protocol was approved by the Animal Care and Use Committee of Shandong University (Approval ref no. 20120907) and was carried out in compliance with the Directive 2010/63/EU on the handling of animals used for scientific purposes [9].
The rats were randomly divided into five groups of 10 rats: control, model, model with positive drug (10 mg/kg captopril), and model with CCE (250 and 500 mg/kg doses). CCE was intragastrically administered daily for 3 weeks. All drugs were dissolved in water before they were given with a 5-mL syringe with a 4-cm-long gavage needle.
Model preparation
After 1 week of acclimatization, the rats were randomly divided into two groups: control and high-fat diet (HFD). The HFD consisted of 40 % fat, 41 % carbohydrate, and 18 % protein for 8 weeks. After an overnight fast, HFD-fed rats were injected intravenously (iv) with a single 30-mg/kg dose of streptozotocin (STZ) (Sigma, St. Louis, MO, USA), while control rats were injected with vehicle citrate buffer. Two weeks after STZ injection, the rats were killed by carbon dioxide suffocation. Blood samples were collected through the tail vein, and plasma glucose levels were measured with a glucometer (Eumed Bio-technology Co., Ltd., Taiwan, China). Rats with fasting blood glucose (FBG) >11.1 mmol/L [10] were selected for the experiment.
Biochemical determinations
Serum samples were collected by eyeball removal, and used to measure total cholesterol (TC), triglyceride (TG), high-density lipoprotein-cholesterol (HDL-c), low-density lipoprotein-cholesterol (LDL-c), serum creatinine (SCr), blood urea nitrogen (BUN), and interleukin-6 (IL-6). Assessments were performed accord to the manufacturer’s protocols for each diagnostic kit (all from Shenzhen Xin-Bo-Sheng Biological Technology Co. Ltd., Shenzhen, China).
Renal cortex assessments
After the rats were sacrificed by cervical dislocation, the renal cortex was homogenized with ice-cold normal saline (W:V = 1 g:9 mL), and the homogenates were centrifuged at 3500 rpm for 10 min at 4 °C. Superoxide dismutase (SOD) activity and malondialdehyde (MDA) and glutathione peroxidase (GSH-Px) levels were measured with commercially available kits (Shenzhen Xin-Bo-Sheng Biological Technology Co. Ltd.) using previously described [11-13].
Urine analysis
The concentrations of albumin and creatinine in urine samples were determined with commercial assay kits (Nanjing Jiancheng, Institute of Biotechnology, Nanjing, China). Creatinine clearance (CCr) and 24-h urinary albumin excretion rate (UAER) were calculated according to the following formulas:
UAER = urinary albumin (l g/mL)/24-h urine volume (mL).
CCr = urinary creatinine (mg/mL)/creatinine in plasma (mg/mL) [14].
Histopathological examination
After the rats were sacrificed by cervical dislocation method, kidney samples were fixed in 10 % phosphate-buffered formalin, dehydrated, and then embedded with paraffin. Sections about 4-μm-thick were prepared from each embedded tissue and stained with hematoxylin-eosin (HE). The prepared slides were examined under a light microscope at 400× magnification by a pathologist who was blinded to the experimental conditions. A 1-mm3 portion of kidney was fixed in 4 % glutaraldehyde in sodium phosphate buffer (0.2 M, pH 7.4) for 3 h at 4 °C. Tissue samples were washed with the same buffer and postfixed in 1 % osmium tetroxide in 0.1 % sodium phosphate buffer (0.2 M, PH 7.4) at 4 °C. The samples were washed with the same buffer for 3 h at 4 °C again, and then dehydrated with graded ethanol. Samples were embedded with resin and polymerized at 72 °C for 48 h. Ultra-thin sections (50-70 nm) were stained with uranyl acetate and lead acetate, and images were captured with a JEM 1200 EX electron microscope (JEM 1200 EX; Jeol, Tokyo, Japan).
Statistical analysis
Values are presented as mean ± standard deviation (SD). Results were analyzed statistically by one-way analysis of variance (ANOVA) followed by Tukey’s multiple comparison using SPSS 16.0 software for Windows (SPSS Inc., Chicago, IL, USA). Differences were considered statistically significant at p < 0.05.
Results
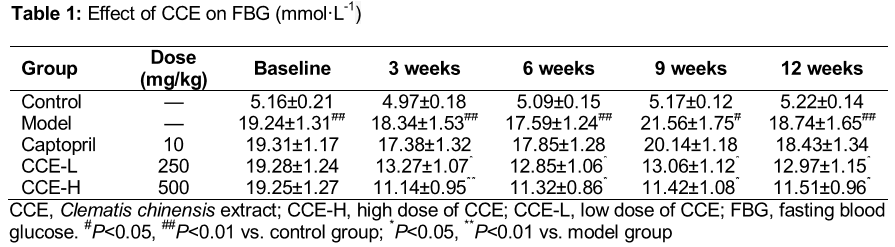
Effect of CCE on FBG in diabetic rats
As indicated in , FBG levels were measured after 12-h fasts at the beginning of the experiment and weeks 3, 6, 9, and 13. At baseline, the diabetic rats had high FBG, which significantly increased throughout the experimental period (p < 0.01). From the third week, CCE (250, 500 mg/kg) significantly decreased FBG (p < 0.05), while captopril (10 mg/kg) had no notable effect (p > 0.05).
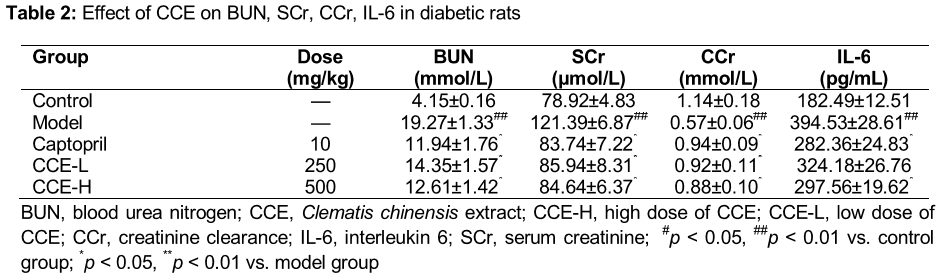
Effect of CCE on BUN, SCr, CCr, and IL-6 in diabetic rats
As indicated in , BUN, SCr, and IL-6 levels were significantly increased in diabetic rats compared to control rats, while the CCr level was decreased (all p < 0.05). Following CCE treatment or captopril treatment, BUN and SCr decreased, while CCr increased (p < 0.05) compared with the diabetic group. IL-6 levels significantly decreased in the high-dose CCE (500 mg/kg) and captopril groups compared with the diabetic group; however, no significant difference was found between the low-dose CCE (250 mg/kg) and diabetic groups.
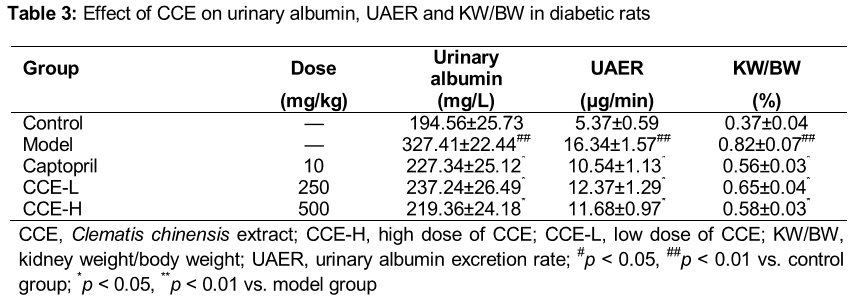
Effect of CCE on renal function markers in diabetic rats
As indicated in , renal function markers, urinary albumin, UAER, and kidney weight/body weight (KW/BW) were all significantly increased in the diabetic group compared with the control group (p < 0.01). CCE (both doses) and captopril significantly reduced urinary albumin, UAER and KW/BW compared with diabetic rats (p < 0.05).
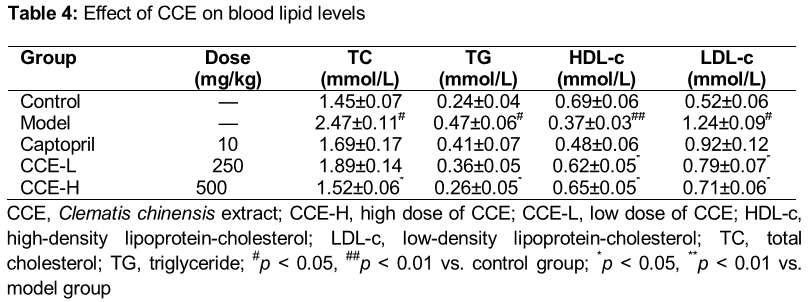
Effect of CCE on blood lipid levels
As in , diabetic rats exhibited hyperlipidemia. Compared with control rats, TC, TG, and LDL-c levels were increased, while HDL-c level was decreased (all p < 0.05). High-dose CCE significantly reduced TC, TG, and LDL-c and increased HDL-c compared with the diabetic group (all p < 0.05). The HDL-c level was increased significantly and the LDL-c level was decreased (p < 0.05) compared with the diabetic group, in the CCE group (250 mg/kg). Captopril treatment did not significantly affect blood lipid levels (p > 0.05).
Effect of CCE on oxidative parameters in diabetic rats
SOD and GSH-Px activities were significantly decreased, and the MDA content in the renal cortex was significantly increased compared with control rats (all p < 0.05). High-dose CCE and captopril normalized SOD and GSH-Px activities and significantly decreased MDA levels (p < 0.05).
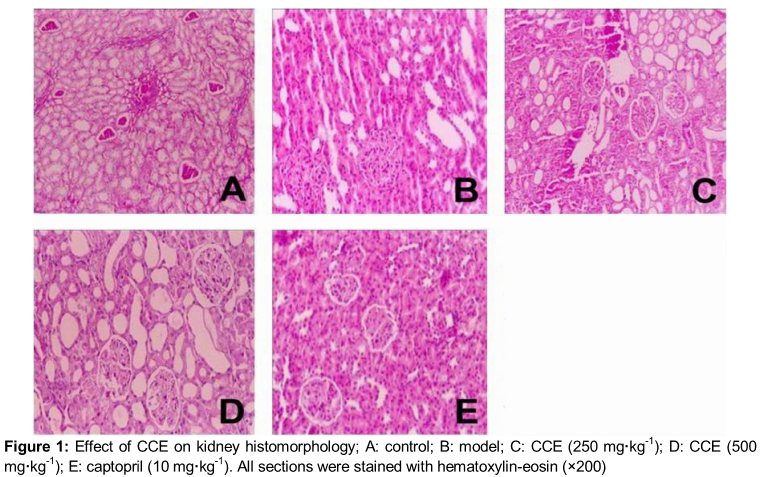
Histopathological features
shows photomicrographs of glomeruli from each group stained with HE. Kidney sections from diabetic rats (b) showed reduced glomerular tuft diameter, balloon adhesion, wall thickening, decreased glomerular volume, tubular vacuolization, and dilation. In contrast, kidney lesions in both CCE groups (c, d) and the captopril group (e) were significantly improved.
Discussion
Our study provides novel evidence of the protective effects of CCE against DN in an experimental model of type 2 diabetes. Consuming an HFD can induce insulin resistance [15], primarily through the Randle or glucose-fatty acid cycle [16]. High TG levels due to excess fat intake can lead to the preferential use of fatty acids for oxidation; this can blunt the insulin-mediated suppression of hepatic glucose output and reduce glucose uptake and utilization in skeletal muscle, leading to compensatory hyperinsulinemia, a common feature of insulin resistance [17-18]. Plasma lipids, insulin levels, and hepatic lipid content are not significantly affected in these animals. An HFD plus a relatively moderate STZ dose can mimic the natural history and metabolic characteristics of patients with type 2 diabetes. We started treating the diabetic rats 2 weeks after STZ injection, which is more reflective of DN in diabetic rats. Hyperglycemia, hyperlipidemia, oxidative stress, and renal injuries all manifested in our model system.
DN is one of the most serious complications of diabetes and is characterized by elevated SCr, BUN, 24 h-UAER, CCr, as well as kidney hypertrophy. Albuminuria is a marker of DN [19], and urinary albumin excretion is considered the best clinical predictor of renal lesions in DN [20]. Creatinine is a breakdown product of creatinine phosphate in muscles, and its clearance is an indicator of glomerular filtration rate. In this study, increased urinary albumin corresponding to the hyperglycemia was notable 13 weeks after diabetes induction. Furthermore, renal function markers CCr, KW/BW, SCr, and BUN were pathologically elevated in diabetic rats. Daily CCE treatment for 13 weeks ameliorated these symptoms of DN progression in diabetic rats.
In the diabetic group, we observed morphological changes including glomerular lesions ultra-structural glomerular endothelium damage, and thickening of podocyte processes and the basement membrane. Histological examination showed that CCE evidently alleviated DN progression. In type 2 diabetes, DN is characterized by dyslipidemia in addition to dysfunctional glucose metabolism. Hyperglycemia enhances glomerulosclerosis and accelerates DN progression. Dysregulation of serum lipid parameters including TG, TC, HDL-c, and LDL-c are common in diabetes [21]. Results of in vitro and in vivo studies strongly suggest that many biochemical and histological abnormalities seen in glomerulosclerosis are analogous to those observed in atherosclerosis [22]. Hyperlipidemia promotes DN development, and diabetes aggravates dyslipidemia [23], perpetuating a vicious cycle. In this study, the diabetic rats showed increased levels of TG, TC, and LDL-c and decreased HDL-c. The lipid metabolites in diabetic rats were improved by high-dose CCE (500 mg/kg).
Some studies have reported that modulating tissue or plasma lipid levels decreases the risks of microvascular disease and related complications [24]. Notably, one group showed that CCE had the potential to normalize lipid metabolism [25]. Accordingly, CCE may prevent DN by ameliorating dyslipidemia.
Uncontrolled hyperglycemia can produce high levels of reactive oxygen species (ROS), which are a major factor in diabetes pathogenesis [26]. Recent studies have confirmed that enhanced oxidative stress and increased ROS production play important roles in many diseases [27]. The human body possesses two types of antioxidant systems: the first includes SOD, catalase (CAT), and GSH-Px, and the second comprises nonenzymatic antioxidant systems. Compared to the DN model group, antioxidant enzyme activities (SOD and GSH-Px) were dose-dependently enhanced in the CCE group, while MDA levels decreased in the renal cortex. These results indicate that CCE could attenuate oxidative damage in the kidney and alleviate DN by increasing antioxidant activities and minimizing MDA production.
Conclusion
CCE can ameliorate kidney damage in diabetic rats. Further studies are needed to clarify the mechanism by which CCE protects against DN; possibilities include glucose regulation, lipid metabolism and oxidative stress, and inflammatory cytokine signaling.
References
Archives


News Updates